More young children with early-onset scoliosis are considered candidates for corrective surgery thanks to new complex surgical pathways that minimize the risk of stunting growth, which has been a longstanding obstacle to early surgery.
Craig Louer, M.D., an assistant professor of orthopaedics at Monroe Carell Jr. Children’s Hospital at Vanderbilt, leads research on interventions for early-onset forms of scoliosis. He has recently compiled case-study summaries on two procedures that minimize vertebral fusion: a hemivertebra excision in a child with congenital scoliosis and the Shilla procedure in a child with syndromic scoliosis.
“While every child is different, we are finding that in many cases, these techniques enable us to control challenging curves that have either failed all other interventions or which would continue to progress and require larger procedures in the future if we didn’t intervene,” Louer said.
Reducing Drawbacks
Infantile scoliosis, diagnosed in children under the age of four, self-corrects in the vast majority of cases, supporting a “wait and watch” approach for younger children with mild curves. Once the child is past 3, however, or when their curve becomes larger than 30 degrees, additional progression is likely and may require treatment with bracing or eventual surgery.
A combination of several technological advancements and guided growth-implant strategies are giving surgeons more confidence in short- and long-term outcomes from corrective surgeries, including hemivertebral resections and rod procedures.
Hemivertebrectomy Reimagined
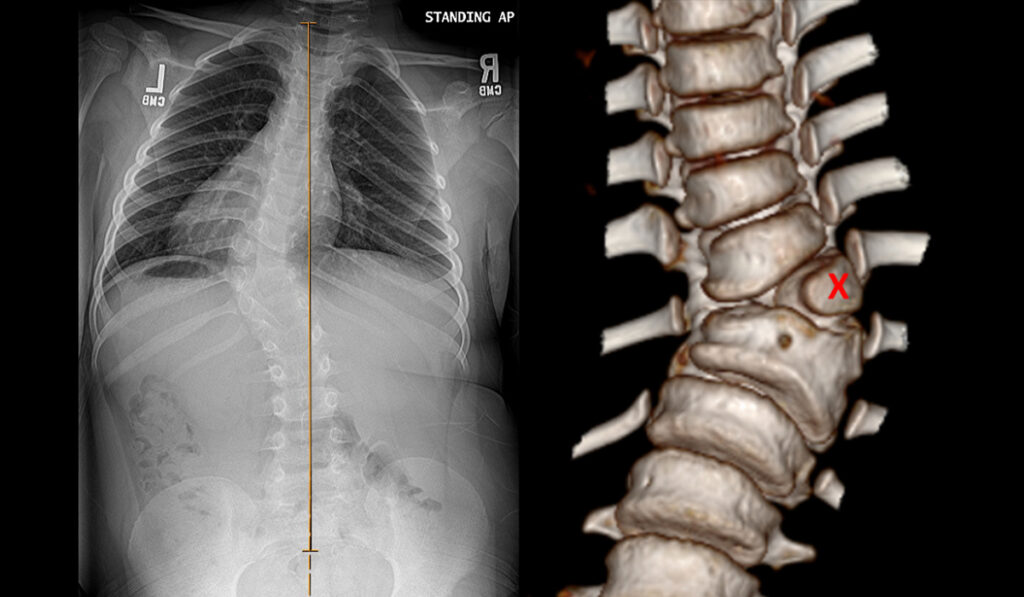
Recently, Louer and co-surgeon Jeffrey E. Martus, M.D., performed a hemivertebrectomy on a 6-year-old boy who had 55-degree curvature secondary to congenital vertebral malformations. His curve had progressed since he was first seen at age 3 and his pain was limiting his ability to play sports. At that point, Louer planned an intervention that would allow for nearly full correction of the deformity by fusing a small number of vertebra and reducing the risk of future deformity in the adjacent spine.
“His spine above and below the fusion were pretty well aligned,” Louer said. “We wanted to make sure that as he continues to grow, those vertebrae adjacent to the middle few that we fused grow with him, and don’t need further intervention.”
From the posterior approach, the surgeons worked around the spinal cord to remove the anterior column of bone and between the lungs with the mediastinum immediately adjacent to their resection. Using a combination of CT navigation and 3D models to guide them, they removed the child’s malformed hemivertebra and fused five adjacent vertebrae.
“These techniques enable us to control challenging curves that have either failed all other interventions or which would continue to progress and require larger procedures in the future if we didn’t intervene.”
Clearer Views, Better Models
Louer says the CT navigation system has been a game-changer in spine surgery, enabling the surgeon to place instruments on the spine and see exactly where they are relative to unique anatomy.
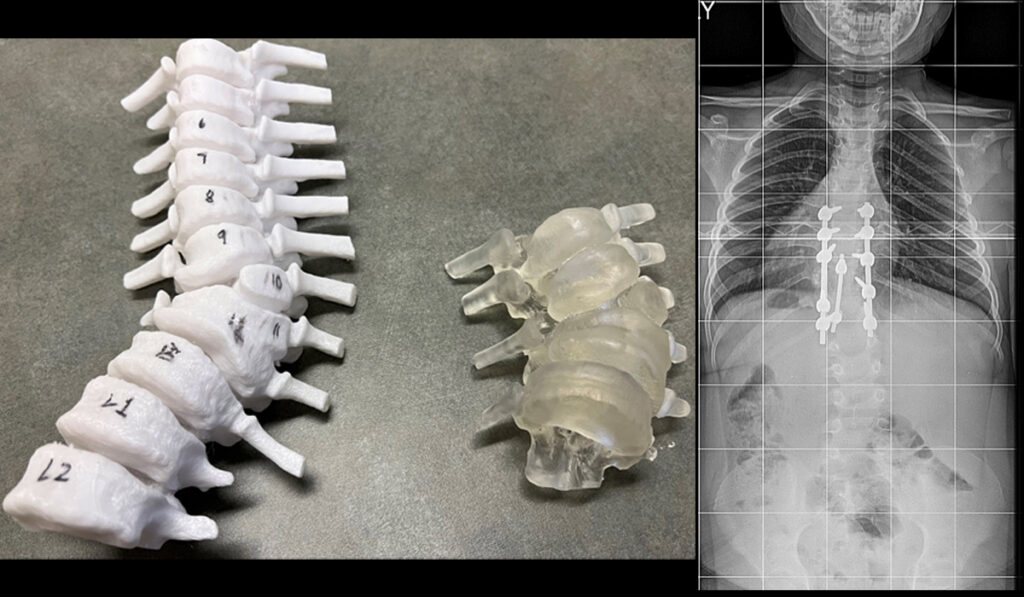
The team also built two printed models – one plastic model they could write on and practice with ahead of surgery, and a second one made of dental resin for use in the sterile operating room.
“It can be difficult to make a mental map in congenital deformities,” Louer said. “Having a 3D representation of the structures involved can improve operative planning, ease of dissection, level confirmation, safe screw placement and bony excision.”
Louer says that these tools boosted his confidence in minimizing the number of vertebrae fused, thus allowing better flexibility and posture.
Room for Growth
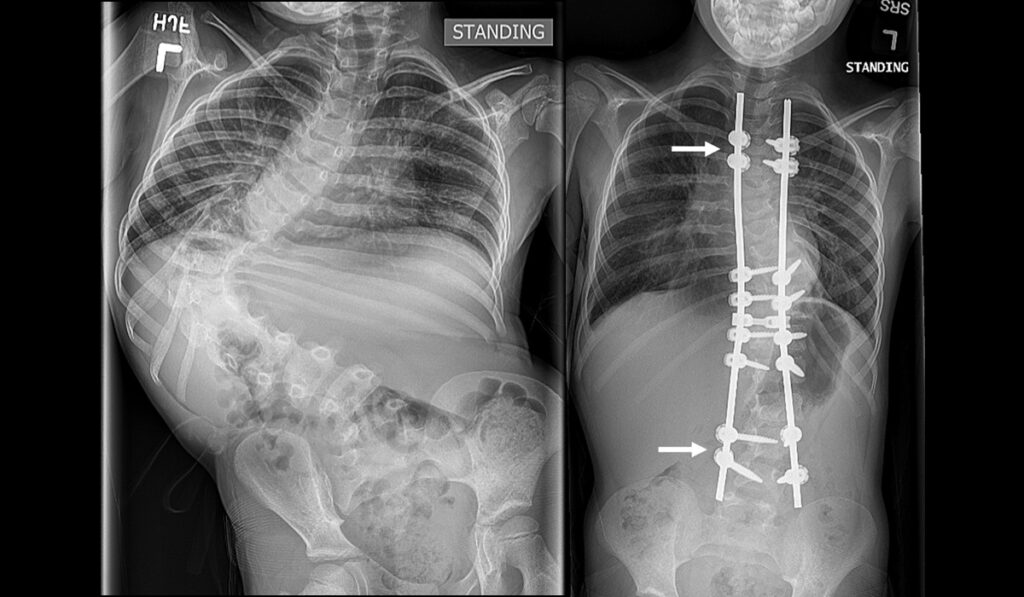
Many principles of hemivertebra excision can be applied to severe scoliosis from other etiologies. Louer and colleagues recently used the Shilla procedure to treat a young patient with syndromic scoliosis measuring more than 120 degrees.
Similar to hemivertebra excision, a small part of the spine was fused at the apex to reduce the most severe section of curvature as safely as possible. In this case, the curvature extended beyond the apex, so the rods were extended to span the remaining curvature and then anchored to non-fused vertebrae via screws. These screws maintain vertebral alignment but allow for sliding along the rod as the spine grows.
“A wide variety of surgical approaches are necessary to treat early onset scoliosis, because the patient population is so heterogenous,” Louer said. “We are excited that with the help of 3D navigational guidance and printed models, we can set more of these children on a path of less pain and lower risk of future surgeries.”