
Today, patients with severe aortic stenosis (AS) can get a transcatheter aortic valve replacement (TAVR) and go home the next day with minimal recovery time. This good news is clouded, however, by the fact that a sizable minority of patients treated with TAVR still die or have persistent symptoms of heart failure that leads to rehospitalization within a year.
“For many patients, waiting until they have symptomatic, severe AS means we come in too late,” said Brian R. Lindman, M.D., medical director of the Structural Heart and Valve Center at Vanderbilt University Medical Center. Lindman and his colleagues are key investigators in randomized, controlled trials, including EARLY TAVR and PROGRESS, which are evaluating the optimal timing for TAVR.
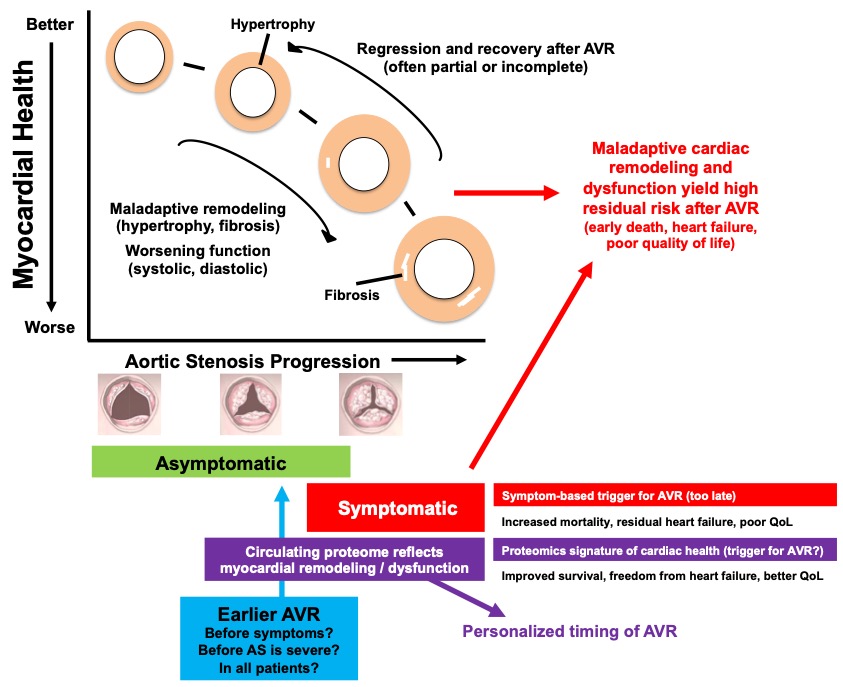
Lindman says the outcomes of these trials may support treating patients with AS earlier, before symptoms develop or even before AS is severe. Further, he believes that circulating proteins will provide insight into heart health and personalize decisions on optimal TAVR timing.
The Rationale for Earlier Intervention
Until almost 15 years ago, the only treatment for aortic stenosis was surgical aortic valve replacement (SAVR). Trials since then have clearly demonstrated that TAVR produces results as good or better than SAVR in patients at all risk levels for aortic stenosis.
“There have been iterative updates and changes in device evolution – such as skirts to prevent paravalvular leaks – that have driven rates of device complications to a very low level,” Lindman said. “This allows us to now tackle questions about optimal timing.”
Lindman’s concern is that patients with moderate AS or asymptomatic severe AS experience chronic pressure overload that causes structural remodeling, fibrosis, hypertrophy and diastolic and systolic dysfunction, problems that are often irreversible or only partially reversible when relieved through valve replacement.
“We have strong evidence that heart dysfunction in many patients is occurring along this journey to severe AS,” Lindman said.
“These patients have a high residual risk of heart failure even after a technically successful aortic valve replacement procedure. Unloading the heart with TAVR or SAVR before irreversible myocardial changes occur might yield a healthier heart and lower residual risk from heart failure.”
Strategy Trials
Lindman is the Vanderbilt site primary investigator for both the EARLY TAVR and PROGRESS trials. EARLY TAVR is enrolling patients with asymptomatic severe AS, and PROGRESS is enrolling patients with moderate AS and symptoms or evidence of cardiac damage.
For both trials, patients are randomized to immediate TAVR or clinical surveillance with deferred TAVR when symptoms develop (EARLY TAVR), or AS becomes severe (PROGRESS). The primary endpoint for both trials is death, unplanned cardiovascular hospitalization or stroke at two years.
Toward Precision Timing
While these strategy trials will provide needed clarity on optimal timing of AVR in patients with AS, some questions will remain. Lindman is the biobank principal investigator for both trials, allowing him and others to study factors beyond the current risk stratification and symptom assessments.
“Guidance on timing of TAVR/SAVR should go beyond assessment of the severity of AS and ascertainment of symptoms,” Lindman said. “The response of the heart to pressure overload from AS – which impacts future risk – varies, and biomarkers measured in the blood may be indicative of a sicker heart, even though the patient is asymptomatic.”
Lindman plans to use a proteomics approach to determine which proteins in what combination reflect the health of the heart and to develop proteomic scores to identify patients who may benefit from earlier valve replacement.
The Sweet Spot
Lindman cautions that no one is lobbying for a wholesale pendulum swing toward early procedures.
“The AS has to at least be severe enough (e.g. aortic valve area <1.5cm2) such that an aortic valve replacement will meaningfully increase the orifice area. Additionally, an earlier replacement runs the risk of leading to more repeat procedures with attendant risks and costs when prosthetic valves degenerate.”
He anticipates that identifying the circulating proteins will be instrumental in personalizing the treatment timing for patients with AS.
“This will allow us to intervene soon enough to mitigate the residual risk of heart failure, while not intervening too soon,” he said.
To learn more about the EARLY TAVR and PROGRESS trials, contact Sarah White at sarah.j.white@vumc.org.



