Physical maneuvers of the sacroiliac joint (SIJ) and posterior pelvis provide minimal information for predicting who will respond to a subsequent diagnostic injection in the SIJ, according to a study in Pain Medicine. The findings contradict the results of some prior investigations supporting the diagnostic use of physical maneuvers.
“Our findings, that the physical maneuvers have very limited predictive power, remove some of the noise and help us get closer to diagnoses that are true,” said first author Byron Schneider, M.D., an assistant professor of physical medicine and rehabilitation at Vanderbilt University Medical Center.
“Our findings, that the physical maneuvers have very limited predictive power, remove some of the noise and help us get closer to diagnoses that are true.”
“This type of work is essential to help guide both clinicians and policy makers as we strive to deliver the best care possible,” added David J. Kennedy, chair of physical medicine and rehabilitation at Vanderbilt and senior author on the study.
Risks of Unneeded Injections
Diagnosing SIJ is notoriously complicated. Initial response to a numbing agent is the most accurate diagnostic available to identify true SIJ pain. However, less than half of patients clinically diagnosed with SIJ pain get immediate relief from the injection. For the remaining patients, there is limited benefit to subsequent treatment with steroid injections.
“Even though the risk with each of these injections is small, millions of people have back pain. At such large numbers, the risks climb and so does the waste of resources,” Schneider said.
Risks from steroid injections include infections at the injection site and injuries to surrounding structures. The medications also disrupt a patient’s hormonal system for weeks, Schneider said, and women who receive excessive amounts of steroids experience an increased risk for osteoporosis.
Injections Versus Physical Maneuvers
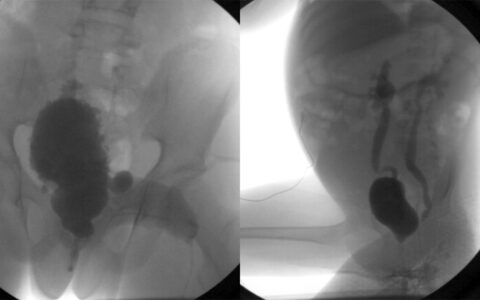
Thirty-nine patients with low back pain enrolled in the study. The patients assessed their pain (using a 1 to 10 scale) just before receiving an SIJ intra-articular injection of lidocaine and a steroid, triamcinolone. Immediately post-injection, the patients again rated their pain.
The researchers also performed six physical exam maneuvers prior to the injection and 15 minutes after the injection.
“The results of these SIJ physical exam maneuvers were evaluated singly and in combination for diagnostic power in relation to a positive anesthetic response (more than 80 percent relief) to the injection,” the authors wrote. In the end, they observed no association between any one maneuver or any combination of them and the patients’ perception of pain relief in response to the injection.
The researchers concluded that the exam maneuvers did not have diagnostic value to identify SIJ pain, as compared to the reference standard of an intra-articular anesthetic block.
Improving Training for Non-surgical Spine Experts
New diagnostic approaches will only be helpful if adopted widely, say the researchers. The North American Spine Society (NASS) is increasing its training efforts around back pain through a new fellowship. “The goal is to fill a void, a kind of no-man’s-land where there have not really been spine specialists who work outside the realm of surgery. We need to train non-operative spine specialists,” Schneider said.
The fellowship represents one aspect of an effort on the part of the NASS to enhance the cooperation of varied medical specialties in the provision of evidence-based spine care. Vanderbilt is participating in this fellowship in interventional spine and musculoskeletal medicine. Schneider is serving as its director, with Kennedy serving as associate director. The contact for more information is associate program manager Kara Dyer (kara.dyer@vumc.org).
“Hopefully as we continue to advance science, we can make better informed decisions for our patients. This combined with a robust training program can only result in better care,” Kennedy said.