
Recent studies by pediatric orthopaedic surgeons at Monroe Carell Jr. Children’s Hospital at Vanderbilt, led by Jon Schoenecker, M.D., are calling into question old assumptions about slipped capital femoral epiphysis (SCFE) etiology. The painful, often immobilizing hip condition occurs in childhood and often leads to hip replacement in young adulthood.
Because children with SCFE are almost always obese, the traditional assumption has been that obesity causes SCFE when excess weight on the hip leads to growth plate failure and slippage. Schoenecker became suspicious of the established theory because obesity is vastly more prevalent than SCFE.
“Although SCFE is associated with obesity, most obese children don’t develop SCFE, indicating that obesity does not independently increase the relative risk of having the disease,” Schoenecker said. “Based on our findings to date, the accomplice appears to be dysregulated leptin production, which is common in many, but not all, morbidly overweight children.”
“Although SCFE is associated with obesity, most obese children don’t develop SCFE, indicating that obesity does not independently increase the relative risk of having the disease.”
Causal Role of Elevated Leptin
Early clues came from their study in children with SCFE and Blount disease (an analogous growth plate dysfunction of the knee). The children with SCFE or Blount – but not obese children without bone disease – had severe hypertension, which impedes proper bone vascularization required for growth plate function.
Hyperleptinemia contributes to hypertension in obese individuals. To connect the dots, Schoenecker and his team set out to discover if the children who had SCFE had elevated serum levels of leptin, and more importantly, if they had higher levels than obese children without SCFE. “The answer was yes on both counts,” Schoenecker said.
“Based on our findings to date, the accomplice appears to be dysregulated leptin production, which is common in many, but not all, morbidly overweight children.”
In a study of 40 children with SCFE and 30 without, researchers found children with elevated serum leptin levels had a 4.9 increased odds ratio of developing SCFE, regardless of obesity, status, sex or race. While leptin level differences were much more marked between the SCFE patients and non-obese controls, SCFE patients also had significantly higher leptin levels than obese controls had.
“Too Much of a Good Thing”
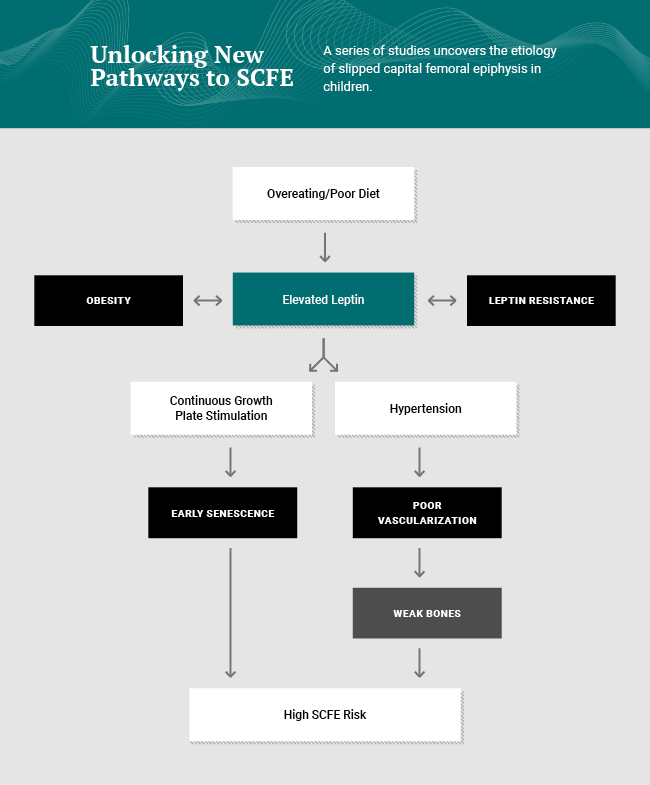
Ninety percent of skeletal growth occurs at night, Schoenecker explained. Normal diurnal pulsed leptin, with increased levels at night is essential for sleep. It promotes satiety needed for fasting and drives bone growth by stimulating the growth plate.
“But, too much of a good thing becomes too much of a bad thing,” Schoenecker said. First the combination of poor diet/obesity over time drives continuous hyperleptinemia. This leads to dysfunctional sleep patterns and hypertension – both of which have deleterious effects on the growth plate and skeletal development. “Ultimately, this can lead to the devastating consequence of SCFE.”
Prevention Through Weight Management
Schoenecker says the timing of SCFE treatment is pivotal in determining mobility, stature, and the adolescent’s surgical fate. “If the slippage is mild, we can secure the hip simply with a screw, and if the child has pain from the deformity, we can usually reshape the femoral head with hip preservation surgery. However, if the slip is severe, or the femoral head loses its blood supply, hip replacement is the only remedy.”
He adds that while pharmaceutical companies are in a sprint to develop drugs that address hyperleptinemia, preventing childhood obesity through education remains the obvious primary goal. “Obesity can be hard for parents to control. They may not get overly concerned about obesity unless they know of tangible negative outcomes,” he said. “Using blood tests to identify kids who are on track toward hyperleptinemia and its symptoms – hypertension, sleep disturbances and abnormal growth – can deliver a wake-up call and gives us a shot at aborting the cascade toward SCFE.”
“Using blood tests… can deliver a wake-up call and gives us a shot at aborting the cascade toward SCFE.”



