Opioid overdose deaths in the U.S. have quadrupled in the last 15 years, an increase that parallels the number of opioid prescriptions dispensed. Pregnant women who deliver via C-section are often prescribed opioids in the hospital for pain and given a prescription for an opioid drug once they go home. These patients are typically given a standard opioid prescription regardless of the quantity of opioids administered in the hospital post-surgery.
In a recent study published in Obstetrics and Gynecology, a group of Vanderbilt University Medical Center investigators set out to evaluate whether individualized post-discharge oxycodone prescribing guided by inpatient opioid use reduces the number of unused opioid tablets after cesarean birth. An earlier study, published in 2017, had characterized post-discharge opioid use and examined factors associated with variation in opioid prescribing and consumption.
“We’ve been using a ‘one-size-fits-all’ approach to prescribing opioids following C-section,” said Sarah Osmundson, M.D, assistant professor of Maternal-Fetal Medicine at Vanderbilt University Medical Center. “This often resulted in unused pills.”
“We first wanted to find out how often and how much these drugs are being used and to determine what we should do at the prescribing level,” Osmundson adds. “Our goal is to prescribe the smallest quantity of opioid drugs possible.”
The Study
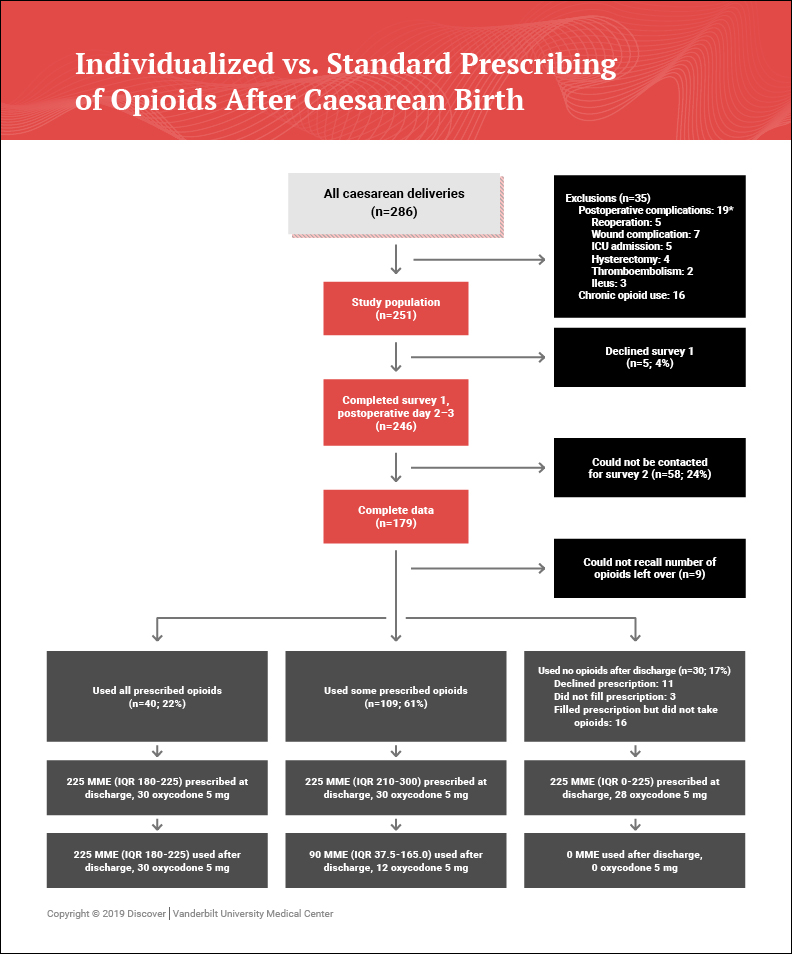
Between June 14, 2017, and August 26, 2017, Osmundson and her co-investigators conducted a randomized, controlled trial of 172 women aged 18 years or older undergoing cesarean birth at Vanderbilt. Participants were randomized at discharge in a 1:1 ratio to a standard (30 tablets of 5 mg oxycodone) or an individualized oxycodone prescription (predicted based on each patient’s inpatient opioid use; median 14 tablets). Baseline characteristics were similar between the groups, as were inpatient pain scores.
All women were contacted starting 14 days after cesarean birth to assess the number of oxycodone tablets used and the adequacy of pain control. The Tennessee Controlled Substance Monitoring Database was accessed to confirm dispensed opioids. The primary outcome was the number of unused oxycodone tablets prescribed for pain control after cesarean birth.
Results of the Trial
Overall, 13 percent (23 of 172) used no opioids after discharge, and 26 percent (44 of 172) used all the prescribed opioids. Women in the individualized group were prescribed fewer tablets (14 versus 30) and had 50 percent fewer leftover tablets (5 versus 10) than women in the standard group. There was no difference in the proportion of opioid used (60 percent versus 61 percent). This was an unexpected finding; if pain were the sole determinant of opioid use women should use the same amount of opioid regardless of study arm. In fact, women used less in the individualized arm that received less opioids on average (8 versus 15). In addition, patient-reported pain outcomes did not differ significantly by group.
Individualized Approach Reduces Unused Pills
“We found that individualized opioid prescribing based on inpatient use reduces both the amount of opioid leftover and the amount used compared with standard prescribing,” said Osmundson. “This study also hints that patient education about proper opioid use could be very important.”
“We usually send patients home with both opioids and ibuprofen. In talking with patients, we’ve learned that there’s a lot of confusion about what they should be taking when they go home from the hospital. One-third of the participants used all their pills because they were simply following instructions on the bottle.”
“My takeaway is that we could decrease opioid prescribing, opioid use, and leftover opioids and still adequately manage pain,” she said. “Since inpatient use correlates with outpatient use, we hope to develop discharge prescriptions customized to a patient’s inpatient use in order to adequately treat pain while minimizing excess prescribed opioids.”